







"Thank you to all the 12th APMEC conference delegates who attended our Early Investigators' Symposium @ APMEC. And to those of you who viewed, and are reviewing the presentation material online on this blog.
As you can see, we had physical constraints due to the layout of the venue, and due to this, several logistic challenges providing enough rooms and outfitting the venues for the many actual and potential conference themes and sessions. There are always two other decision trade-offs at any large conference - to choose between two or more equally interesting sessions, and the limited time available for presentation and discussion. I hope this blended face to face, and online approach to address some of these challenges has helped address some of your learning and information needs.
For my presentation, I opted to provide as much background, practical and practice information through this blog before the session. This allowed the live session to focus on an attempt to customise the actual presentation to my perceived needs of the on site audience via live "raise-hand" polling. I sincerely hope the presentation focus on key take home (translatable) points, embodied in the "thank you slide" at the beginning of the presentation, as well as in the presentation abstract, has been useful for you. We were then able to allocate much longer time to live discussion of questions raised by the audience, rather than spend this time on a "didactic" presentation.
The screenshot below shows the "actual" formal presentation material.
Audience questions raised during the live Q and A session related to finding time for educational scholarship, the practical issue of developing and refining a research question, and the role of clinicians and clinician scholars in the educational research process. I will elaborate on these questions further in the rest of this week.
(This section was written and posted at 0800hrs, Monday, Feb 9th, 2015; during the analysis, reflection, and early dissemination phase of the educational scholarship cycle applied to this symposium presentation. Very best, Poh-Sun)

Screenshot of the "actual presentation" given from the upper right-hand section of the Padlet digital wall (click this link for the website) due to real-time customisation of the presentation following live "raise hand" polling of audience











http://padlet.com/dnrgohps/pracmededres (the Symposium presentation interactive Padlet digital wall website link)








(CBD = Case-based discussions)
Above from Khan & Ramachandran (Medical Teacher, 2012 link to paper below)
.jpg)



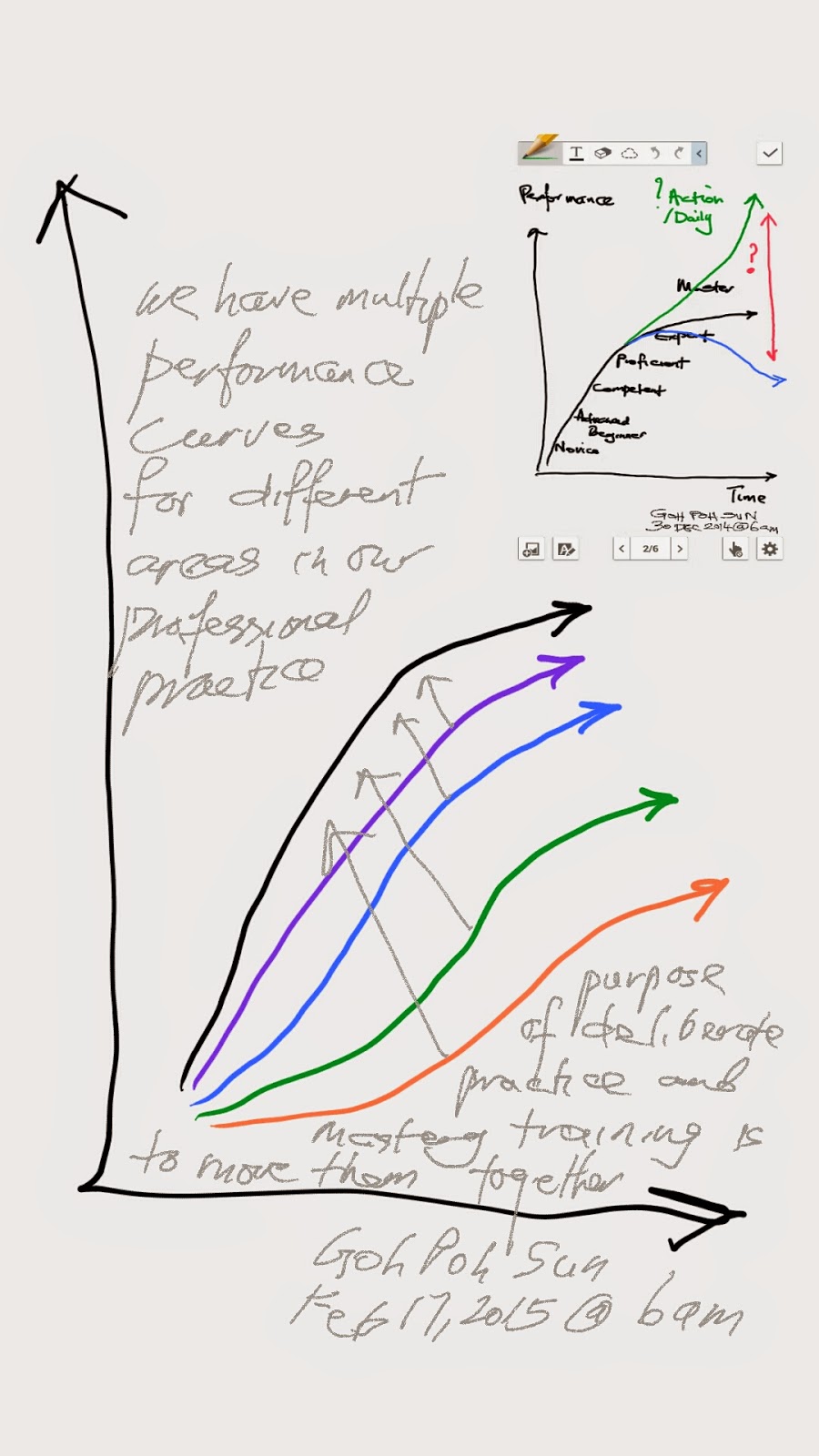
Work on one curve systematically and in sustained manner. Then next curve. Commit to share (presentation, lecture, symposium, educational exhibit, paper) to not only motivate yourself, but also as a learning and integrative exercise. (Shared with Associate Consultant as tip for continuing professional development, Feb 16, 2015).


.jpg)






Chapter 4 (above) in



Scholarship, publication, and career advancement in health professions education: AMEE Guide No. 43.

'The research compass': an introduction to research in medical education: AMEE Guide no. 56.

Medical education scholarship: an introductory guide: AMEE Guide No. 89.








Re-imagining a medical and postgraduate training curriculum by integrating online with face to face learning and interaction - a PhD proposal / example of a program of medical education research
by Dr Goh Poh Sun
MBBS(Melb), FRCR(UK), FAMS(Singapore), MHPE(Maastricht)
Background
Professional training programs are faced with the constant challenge of exponentially increasing curricular content, or curricular "bloat", crowding out curricular time allocated for student interaction and content assimilation, not to mention content integration.
The paradox is that professional training programs are lengthy multiyear, if not decade long training and apprenticeship encounters. As educators, we have not taken full advantage of the potential of educational technology to provide access to comprehensive, standardised, peer-reviewed, high quality content for both students, and instructors; during this lengthy training process. To revisit, and build upon fundamental principles and case-based experience; utilising the best available educational theory, including mastery training and deliberate practice principles, evidence from the literature, as well as local empirical experience. We have also not taken full advantage of the potential of educational technology and eLearning to make our teaching public, scholarly, and a showcase of educational scholarship.
In the next 5 studies, as part of a "PhD level" educational proposal, the role of educational technology, eLearning or technology enhanced learning will be reviewed in the context of a longitudinal medical training program, spanning the undergraduate, through postgraduate, to continuing professional development and lifelong learning settings. A series of studies will be proposed to evaluate, assess, and measure the impact of these educational efforts in revising a training curriculum.
Study 1 and 3 - eLectures vs traditional Lectures in undergraduate (study 1) and postgraduate (study 3) medical education
Lectures can (1) provide an efficient and time effective way to share complex information with large groups of students in an enthusiastic and engaging way; (2) present a framework to facilitate understanding and provide an introduction and overview of complex topics, helping integrate prior knowledge with current information for students; (3) customise the material for a specific cohort of students to address their learning needs; (4) be used to provoke thought and deepen understanding; and (5) be used to promote independent learning (Brown & Manogue (2001); Exley & Dennick (2004).
eLectures possess many of the advantages of traditional lectures; with the added functionality and advantage of widening access to high quality standardised peer reviewed content to both students and instructors; to learn from, and build upon (see background section).
A key advantage of making eLecture content available, in both packaged, and granular form (by indexing key take-home points, key tables and graphics and important references and review papers for example); is that students can review and revisit principles, and illustrative case studies repeatedly through their longitudinal training program (with timing and sequence both guided by instructors in an adaptive curriculum; and also on demand as and when required by students). This reinforces basic principles; and improves transfer (Baldwin & Ford,1988). The provision of eLecture content which students engage with repeatedly promotes learning.
eLectures can facilitate self-directed learning in students. eLectures offer curricular planners and educators greater flexibility to deliver and customise educational content, and facilitate an adaptive curriculum.
There are several ways we can evaluate and assess these assertions.
For example, for students, we can measure time to competency for undergraduates as an index for efficiency. We can measure time to proficiency, and mastery for postgraduates; as an index for efficiency. For both undergraduates, and postgraduates, we can assess understanding, knowledge retention, and ability to apply key ideas and principles as an indicator of effectiveness. For instructors, we can measure lecture preparation time as an index for efficiency. And assess the relative ease of evaluating teaching effectiveness using eLectures vs traditional lectures.
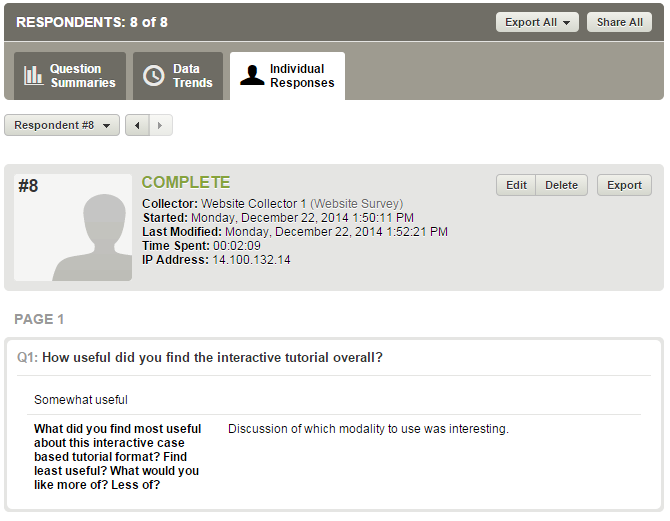
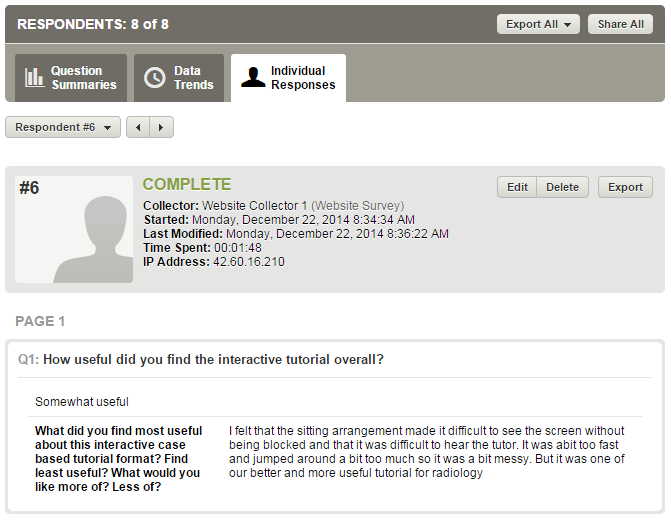
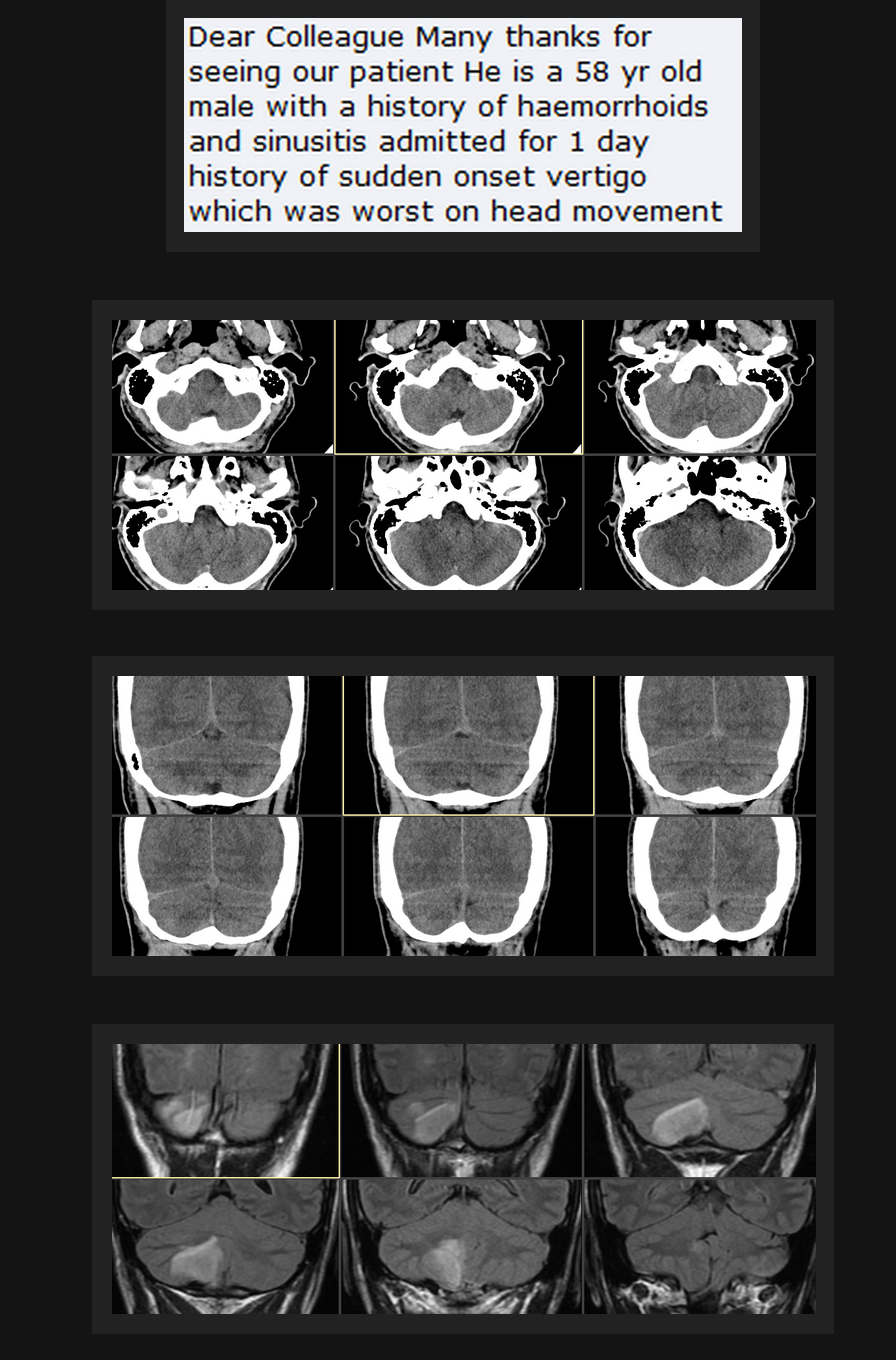
Study 2 - role of interactive eCases in undergraduate medical education
What is the role of interactive eCases in undegraduate medical education? Presenting typical examples of common clinical conditions serves to illustrate principles and key ideas introduced in the basic science units of a medical curriculum. More significantly, these clinical scenarios and case examples are the starting point of future clinical encounters, and serve as both knowledge anchors around which deeper experience can be built with exposure to further clinical case examples, as well as triggers to recall key practice points, while deepening understanding of basic science principles.
"Previous research has shown that physicians make a diagnosis from the patient’s history in 70-90% of cases, i.e., while medical student consider the correct diagnosis based on the chief complaint or the history in 70% of cases." citing
(1. Gruppen LD, Woolliscroft JO, Wolf FM. The contribution of different components of the clinical encounter in generating and eliminating diagnostic hypotheses. Res Med Educ. 1988;27:242-7.
2. Peterson MC, Holbrook JH, Von Hales D, Smith NL, Staker LV. Contributions of the history, physical examination, and laboratory investigation in making medical diagnoses. West J Med. 1992;156(2):163-5.
3. Gruppen LD, Palchik NS, Wolf FM, Laing TJ, Oh MS, Davis WK. Medical student use of history and physical information in diagnostic reasoning. Arthritis Care Res. 1993;6:64-70.) from
The contribution of the medical history for the diagnosis of simulated cases by medical students Tomoko Tsukamoto, Yoshiyuki Ohira, Kazutaka Noda, Toshihiko Takada, Masatomi Ikusaka (International Journal Medical Education. 2012;3:78-82)
Students are progressively exposed to clinical scenarios illustrated with key points in the clinical history, physical examination findings, laboratory data and clinical imaging findings.
This process of building a firm foundation of clinical case based scenario recognition ("think fast", pattern recognition, or "what") supported by a firm foundation of increasing deeper understanding of basic science principles ("think slow" or "why") is fundamental to developing both forms of clinical reasoning, giving future clinicians the ability to quickly recognise common and important clinical scenarios, as well as the capacity and ability to reason from first principles with atypical clinical presentations, with less defined, multiple and conflicting clinical features.
Study 4 - role of interactive eCases in postgraduate medical education
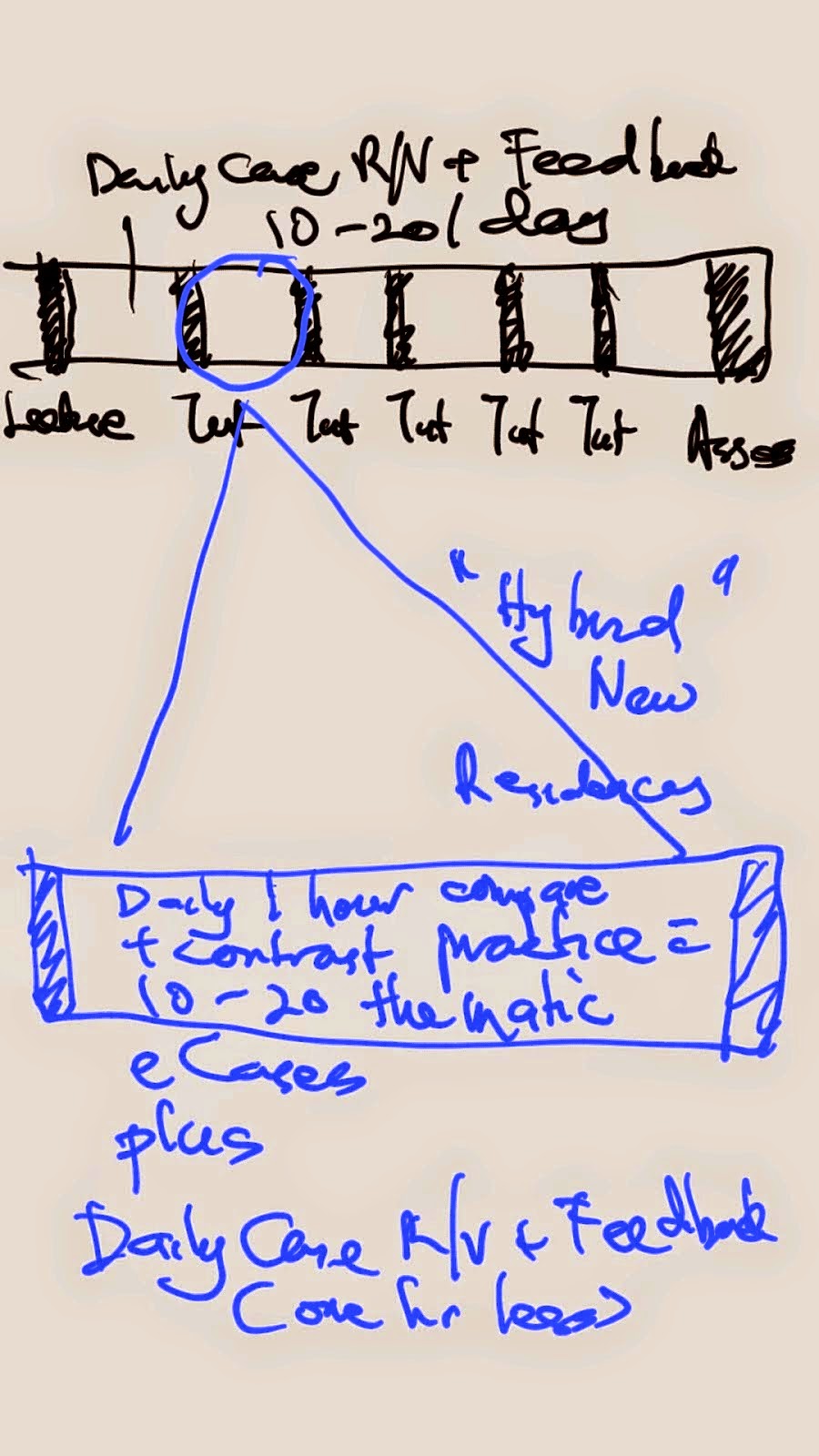
Re-imagining a postgraduate training curriculum
A combination of eLectures (e=online; e=edited, 0.5 time traditional lectures), daily deliberate practice sessions with theme based interactive online sets of clinical cases for compare and contrast practice coupled with online and regular face to face feedback and discussion with clinical tutors; together with supervised daily clinical sessions with clinical teachers in a coaching role; augmented by individual resident ePortfolios for formative assessment and self reflection; can potentially dramatically reduce the training time required in postgraduate training programs, delivering a more personalised educational experience, focused on identifying an individual trainee's strengths and augmenting these, as well as strengthening areas of weakness in performance.
Study 5 - role of a hyperlinked indexed eRepository in continuing medical education
Learning@NUHS
Using a digital knowledge repository to personalise learning in medical education - a follow up report (to TeL 2013) (TLHE 2014 oral presentation paper)
Building an online repository of teaching resources to facilitate consistent and good quality teaching of postgraduates and undergraduates in medicine – a preliminary report (TeL2013 oral presentation paper)
Use of case pairs can potentially improve the efficiency and effectiveness of radiology residency (MHPE Master Thesis, June 2012)
Review of studies and PhD thesis












Impact and Case Studies






Scholarship.jpg)









compare with http://eurorad.org/ screenshot below

and compare with http://radiopaedia.org/ screenshot below


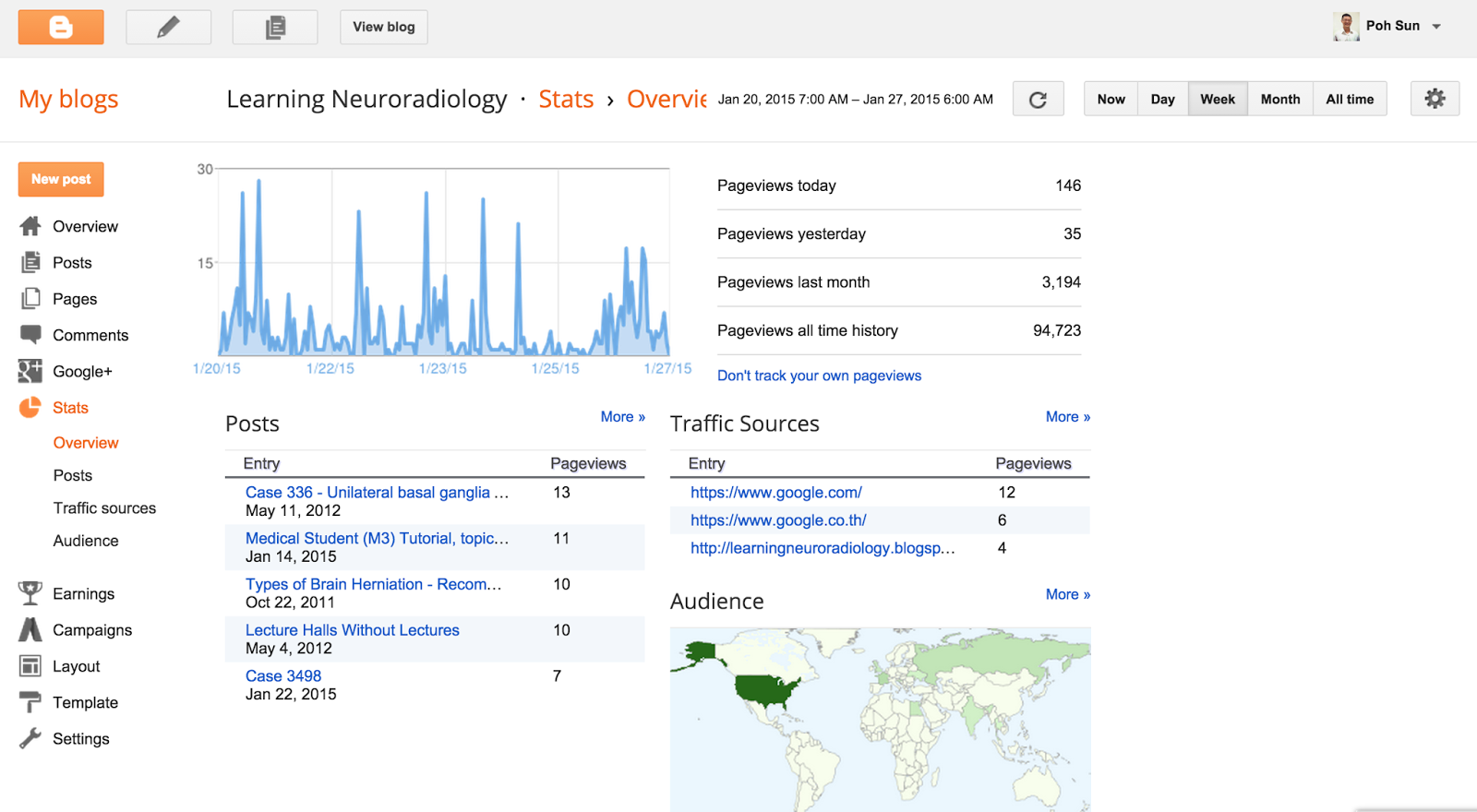
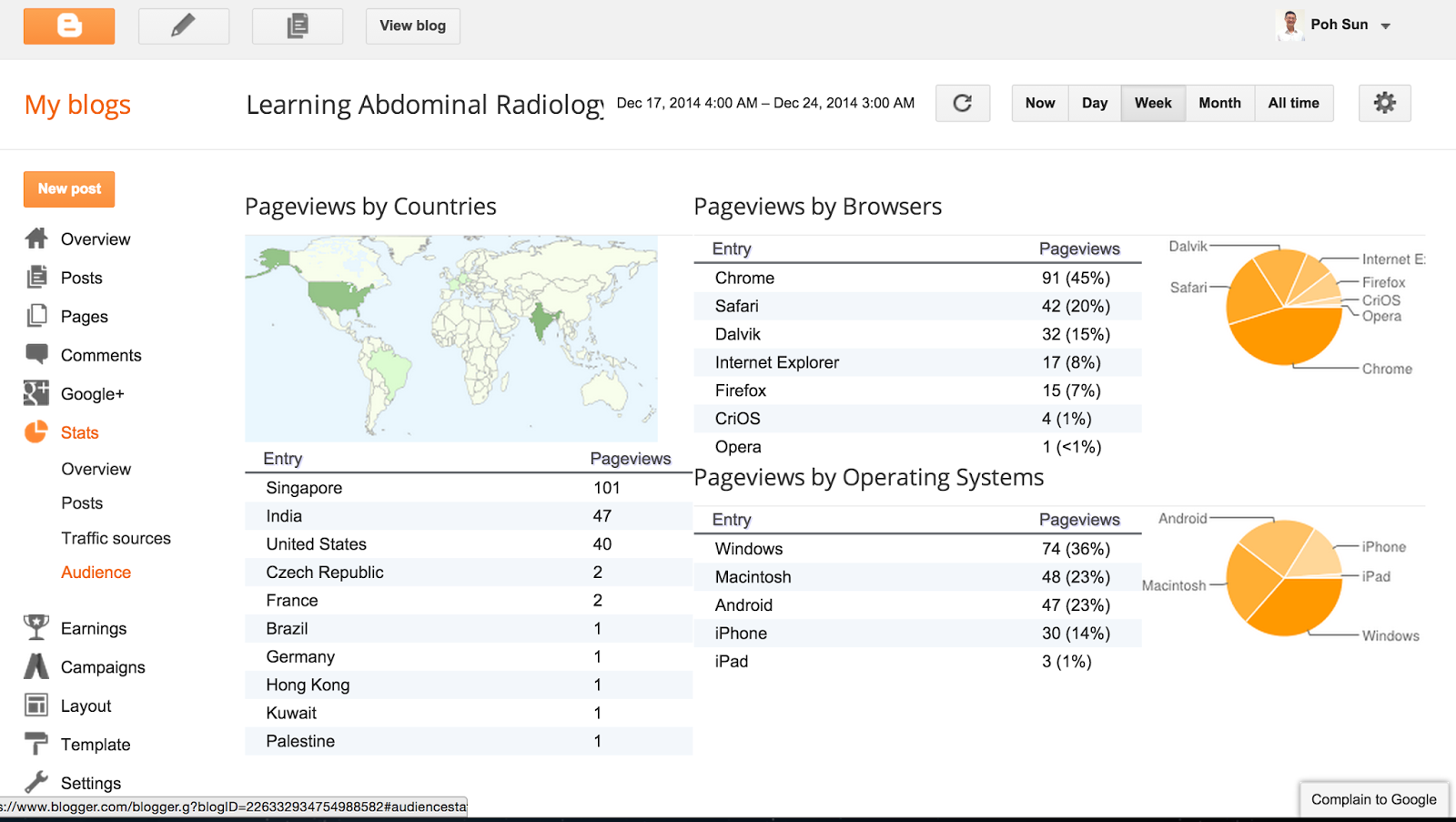
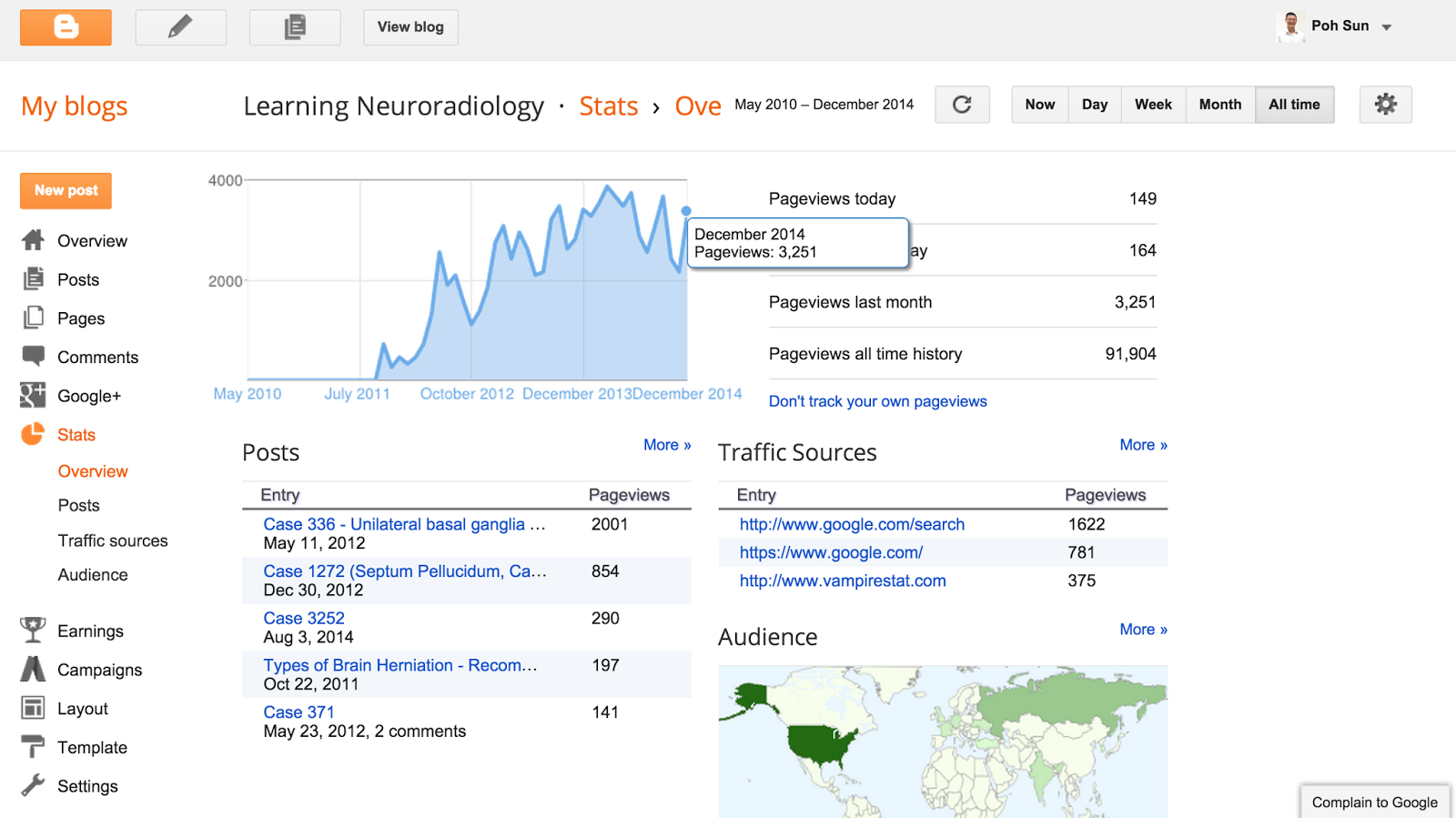
Upcoming CenMed workshops (above). eLearning workshop (Technology enhanced learning workshop) in 5th year; other workshops piloted last year in 2014). Content for MEU, now CenMed workshops are delivered via MedEd blog. Viewership stats below.








(Selected recent conference paper presentations above)



(Accepted for publication on Feb 11, 2015)







.png)













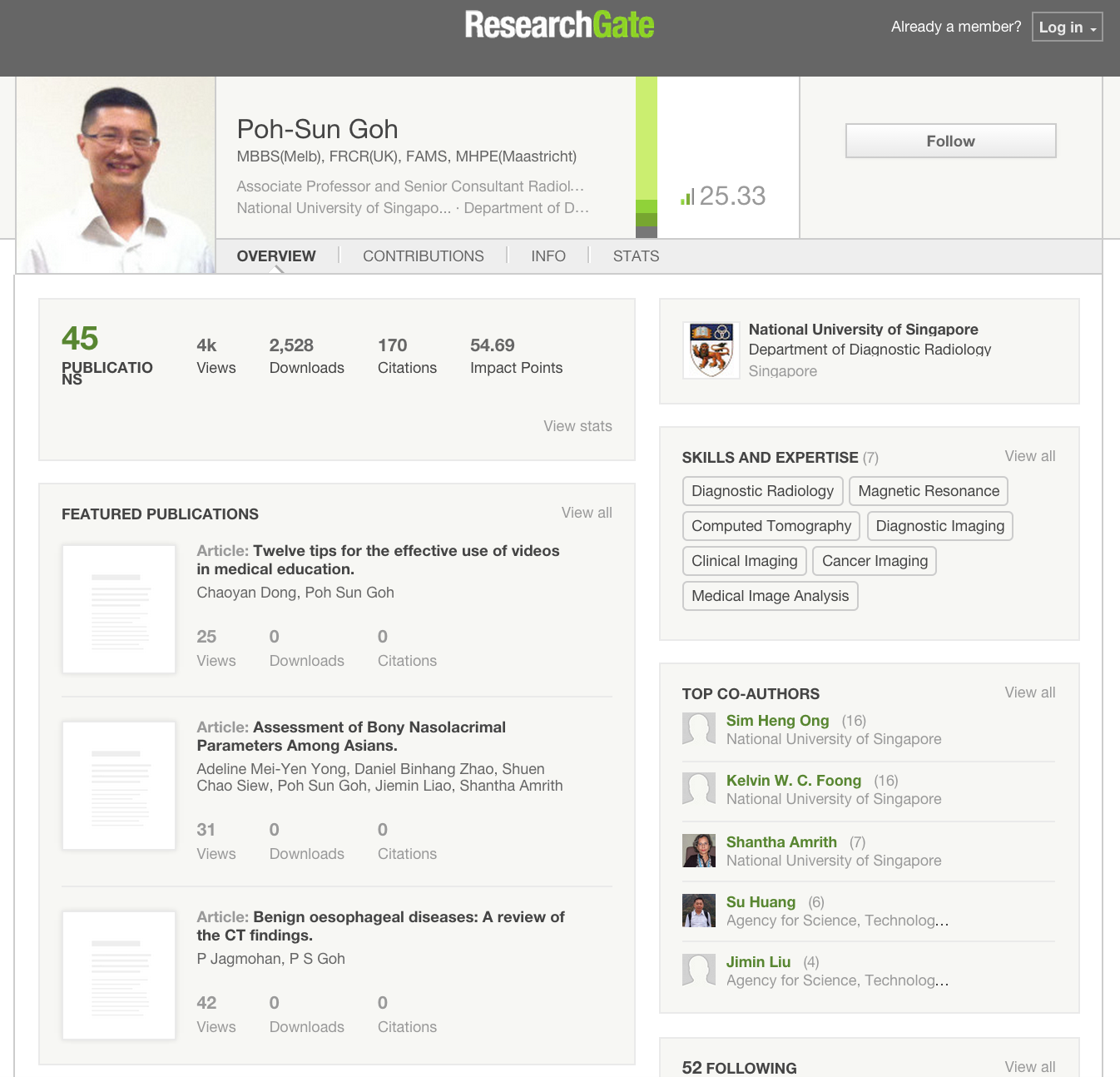
(See bottom of this webpage for more publications)










vs















above illustration from http://www.servicelearningcourse.org/image/pyramid.gif
{kind=link}

above illustration from http://www.searchcowboys.com/images/upload/how-we-learn-seo.jpg
{kind=link}


Scholarship.jpg)




(CBD = Case-based discussions)
Above from Khan & Ramachandran (Medical Teacher, 2012 link to paper below)
.jpg)




The following is screenshot image is excepted from the LinkedIn profile of the Prideaux Research Centre, Health Professions Education, Flinders University, Adelaide, Australia














































































vs











Use of case pairs can potentially improve the efficiency and effectiveness of radiology residency from Poh-Sun Goh

























(above 2 images screenshots from AJNR Case of the Week menu pages)

(above screenshot from ASNR-Neurocurriculum Live eLecture program)



(above and below screenshots from StatdX online reference tool)










.png)




















Impact and Case Studies


compare with http://eurorad.org/ screenshot below
and compare with http://radiopaedia.org/ screenshot below
(Selected recent conference paper presentations above)
Upcoming CenMed workshops (above). eLearning workshop (Technology enhanced learning workshop in 5th year; other workshops piloted last year in 2014). Content for MEU, now CenMed workshops delivered via MedEd blog. Viewership stats below.
(Accepted for publication on Feb 11, 2015)











Selected radiology conference papers (above)



.png)
also see




















Digital Analytics Fundamentals (4 to 6 hour interactive online course from Google Analytics Academy)




Additional faculty development resources below:
Thanks for picking out the time to discuss this. It is extremely helpful for me.Thanks for such a valuable help again.
ReplyDeleteRead More About : recruitment agency singapore